Introduction
The Common Vein 2010
Definition
Thyroid cancer is a malignant condition usually with no known cause, but sometimes associated with radiation exposure and in patients who are genetically predisposed.
Structurally the disease usually manifests with a non functioning thyroid nodule. Lymphadenopathy is present in later stags of the disease.
Types of thyroid cancer
Papillary Carcinoma (75-85%)
Follicular Carcinoma (10-20%)
Medullary Carcinoma (5%)
Anaplastic Carcinoma (<3%)
Other – squamous type, lymphoma
Clinically the patient usually presents with a nodule. Causes for concern include age of the patient (younger patients more likely to have malignant disease) , family history of thyroid cancer and excessive radiation exposure, particulalrly if exposure during childhood.
Imaging is by ultrasound examination and concerns for malignancy are raised when there are microcalcifications, thick irregular halo or irreular margins of the mass. Malignant lesions are usually hypoechoic and often hypervascualr in the matrix. Fine needle aspiration under ultrasound guidance is performed on any lesion with concerning ultrasound characteristics or in a patient with a high clinical suspicion of thyroid cancer.
The diagnosis is suggested or confirmed by pathologic examination.
Treatments include thyroidectomy or lobectomy. Radioactive iodine 131 is used in patients with papillary and follicular cancer for ablation of residual thyroid tissue after surgery but also for carcinoma that shows uptake of iodine.
|
Suspicious Nodule |
|
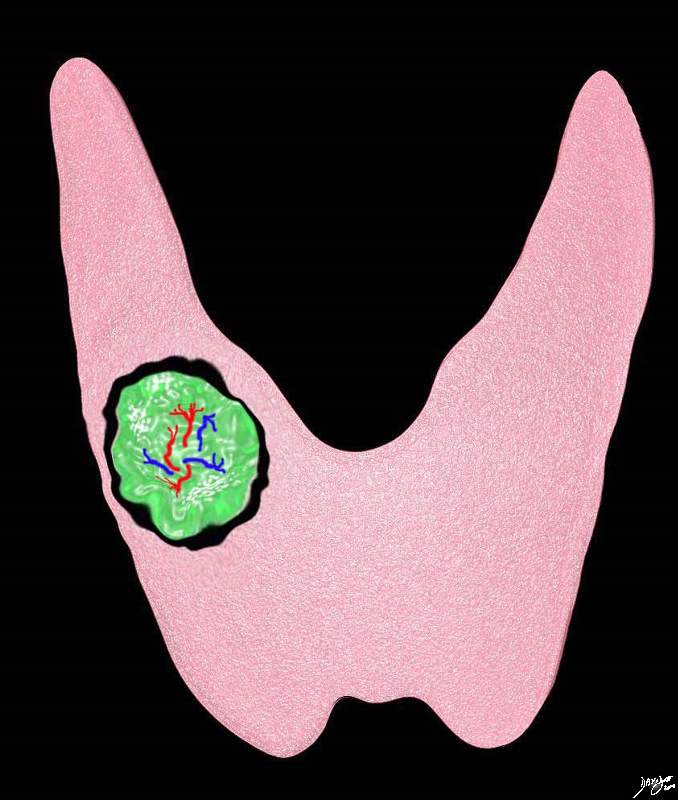
The diagram outlines a nodule in the right lobe of the thyroid serves to illustrate the features that are concerning for malignancy on ultrasound examination. These features include irregular or focally thickened halo((black), and or irregular margin of the nodule. Of lesser importance is central hypervascularity microcalcifications (white speckles). Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 93852.d11b02g01.8s |
Irregular Margin (green arrow) |
|
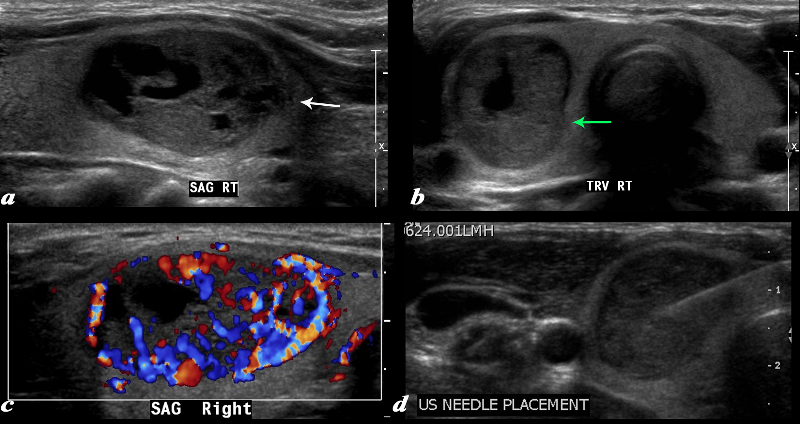
A large complex mass occupies more than half the right lobe of the thyroid gland is seen by ultrasound. The mass measures 2.6cms in sagittal and in A-P dimension measures 1.7cms(a). In transverse it measure 1.7cms. It is characterized by a mildly hypoechoic matrix with cystic type serpiginous components. (a) The margins are irregular (white arrow, a) There is an incomplete halo which shows regions of irregularity (green arrow) The lesion is extremely vascular both peripherally and centrally (c) A biopsy was performed and showed medullary carcinoma. Courtesy Barry Sacks MD Copyright 2010 97339cL01.8 |
Irregular Wall and Microcalcifications |
|
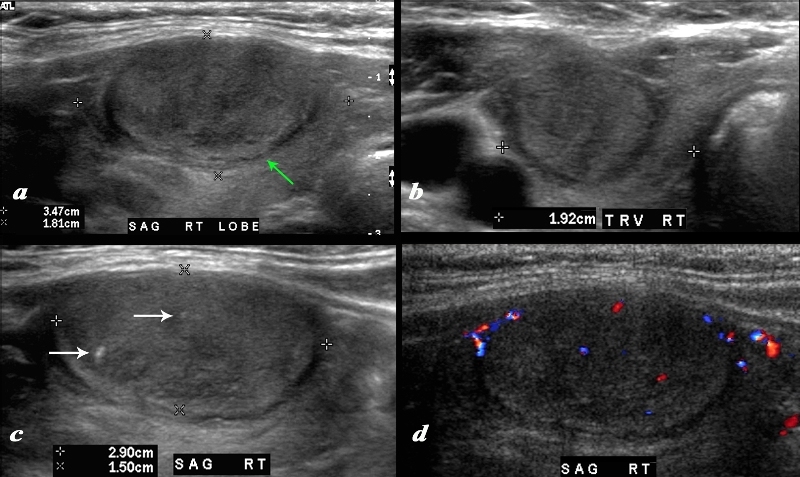
A large nodule in the thyroid occupies almost the entire right lobe (a). The nodule measures 2.9cms by 1.5cms. The gland is not enlarged and measures 3.5cms (craniocaudad), by 1.8cms (A-P) by 2.4cms (transverse). The nodule is almost isoechoic with normal thyroid but shows internal irregular areas of hypoechogenicity, regions of isoechogenicity, as well as microcalcifications (white arrows (c). There is irregularity of the border at the posterior aspect of the nodule green arrow a). The halo shows irregular borders in this region as well. Internal vascularity is minimal (d). The irregular surface is concerning for a malignant processes. The diagnosis in this patient was papillary carcinoma Courtesy Ashley Davidoff MD Copyright 2010 74909c02L.8 |
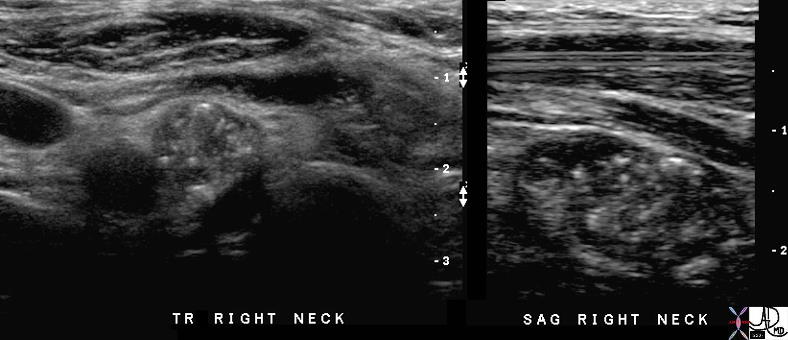
Thyroid Metatstases in Lymph Nodes Revealing Characteristic Microcalcifications |
| The patient has a history of papillary thyroid carcinoma treaeted 16 years ago. The transverse and sagittal image of a cervical lymph node that is heterogeneous with multiple punctate shadowing microcalcifications. These findings are consistent with recurrent papillary thyroid carcinoma.
Image Courtesy Ashley Davidoff MD Copyright 2010 70982c01 |