The Common Vein Copyright 2010
Definition
Hurthle cell neoplasms, which can be benign or malignant, are thyroid lesions defined generally as ontaining at least 75% Hurthle cells. Distinguishing benign from malignant Hurthle cell neoplasm is not possible by fine-needle aspiration alone. Hurthle cell carcinomas are considered a more aggressive variant of follicular carcioma of the thyroid and are labelled follicular carcinoma, oxyphilic type.
Cause of Hurthle cell neoplasm is unknown. While some suggest a progression from bening adenoma to cancer in Hurthle cell neoplasms, this scenario has not been proven. Hurthle cell formation seems to be a metaplastic phenomenon that occurs more frequently in inflammatory disorders like thyroiditis, or other situations resulting in cellular stress. Genetic mutations and a history of radiation to the neck are risk factors for Hurthle cell carcinoma.
Hurthle cell neoplasms result in an encapsulated lesion that may be cancerous.
Structurally these lesions are hypercellular with an abundance of large polygonal Hurthle cells. These cells in the thyroid contain abundant eosinophilic granular cytoplasm as a result of accumulating altered mitochondria. They have a large nucleus and nucleolus. The proliferation of oncocytes gives rise to hyperplastic and neoplastic nodules.
Functionally these neoplasms have a variable rate of malignancy, but generally higher than most thyroid nodules, ranging up to 65%. There is a sense of reported mortality rates higher than that from other thyroid cancers.
Clnically Hurthle cell neoplasms can present as palpable thyroid nodules, or found on thyroid ultrasound. Symptoms of larger masses, included dysphagia and choking, heighten the risk of malignancy. As a subtype of thyroid cancer, Hurthle cell cancers are rare, accounting for fewer than 10%.
Imaging is performed by ultrasound to detect size of lesion. Lesions are usually solid masses. Frequently cancers are bilateral. MRI or CT may provide more detailed information abou tthe tumor and other neck structures. Radioactive iodine uptake is generally decreased in a Hurthle cell neoplasm.
Diagnosis of Hurthle cell neoplasm is made by fine needle aspirate, although diagnosis of carcinoma can only be made by vascular and capsular invasion.
Treatment of Hurthle cell neoplasm is surgery. all patients with cytologically diagnosed HC neoplasms should undergo resection of the thyroid gland, often total thyroidectomy. Levoxine therapy is begun post-operatively.
Homogeneous Nodule |
|
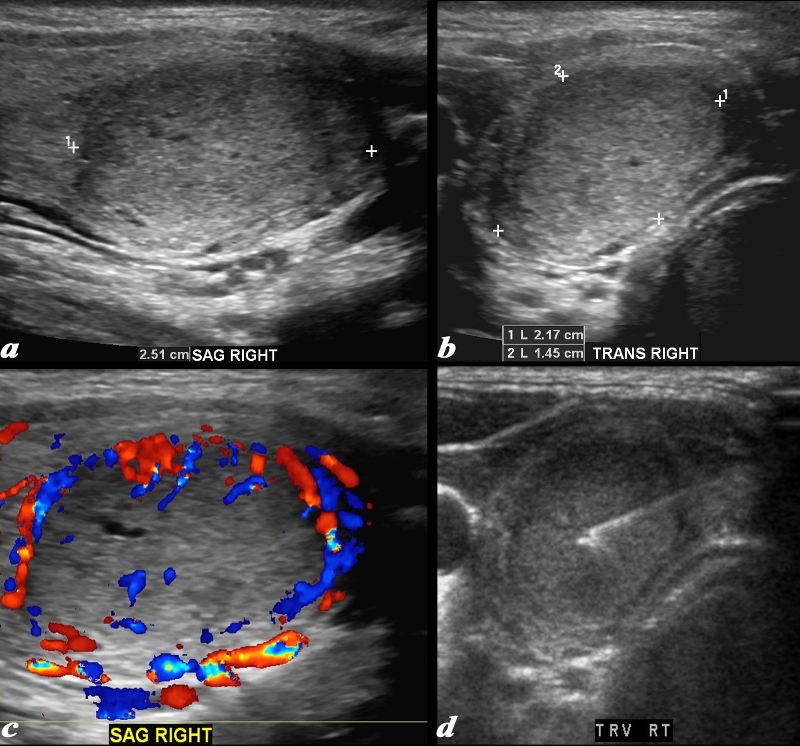
This ultrasound is from a female patient who presents with a thyroid nodule. Ultrasound shows a mass in the right lobe of the thyroid. The nodule measures 2.5cm in sagittal (a), 2.2 cm in A-P dimension (b) and 1.5cm in transverse view. The mass is isoechoic to hyperechoic, is mostly homogeneous, but for tiny cystic spaces with Doppler flow that is mostly peripheral but does have some central flow as well (c). Image (d) shows a well placed aspiration needle. A diagnosis of Hurthle cell neoplasm was made. Courtesy Barry Sacks MD Copyright 2010 97073cL.8 |
|
Hurthle Cell Carcinoma |
|
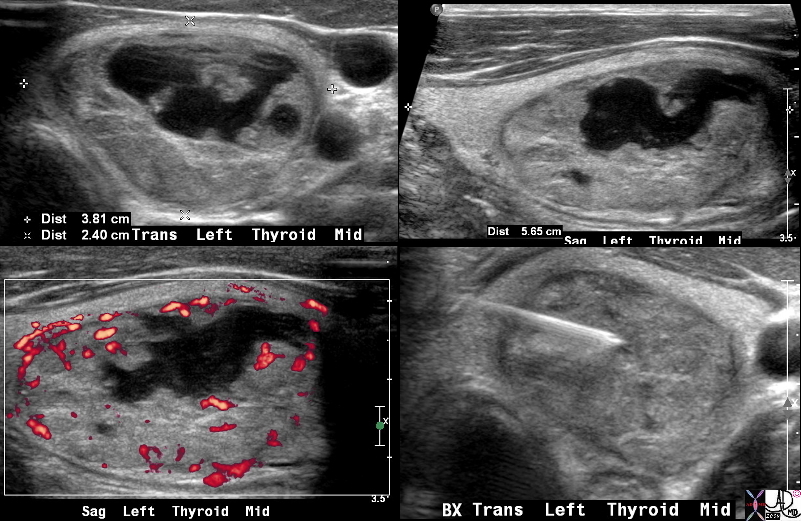
This is a thyroid scan from a 31 year old female with a clinical history of a thyroid nodule. The scan shows a heterogeneous and complex mass involving almost the entire left lobe that is well defined both on the transverse view (a) as well as the sagittal view (b). The left lobe measures 5.7X 3.8 X 2. 4 cms, resulting in a grossly enlarged left lobe as a result of the mass. An serpiginous cystic appearing component is seen in images a,b,and c and contains complex fluid and nodular excrescences. Blood flow is mostly on the periphery with the cystic component being avascular. A biopsy was performed (d), which revealed a Hurthle cell carcinoma Courtesy Barry Sacks MD Copyright 2010 99394c.8s |
—
References
Zeev V. Maizlin, MD, Sam M. Wiseman, MD, Parag Vora, MBBS, John M. Kirby, MB, BCh, BAO, Andrew C. Mason, MD, Douglas Filipenko, MD and Jacqueline A. Brown, MD Hürthle Cell Neoplasms of the Thyroid Sonographic Appearance and Histologic Characteristics J Ultrasound Med 27:751-757 2008