The Common Vein Copyright 2010
Definition
Follicular Carcinoma is a primary malignancy neoplasm of the follicular cells in the thyroid gland. It is a well-differentiated carcinoma that is difficult to distinguish from benign follicular adenomas. Follicular CA is the second most common malignancy of the thyroid gland.
Follicular Carcinoma of the thyroid is caused by genetic mutations, especially of the ras oncogene, resulting in malignant transformation of follicular cells . Ionizing radiation has been associated with several thyroid malignancies, including follicular carcinoma.
Structural changes of the thyroid gland include nodule or mass formation and growth. Histologically, Follicular CA can be encapsulated and difficult to distinguish from a benign follicular adenoma although blood vessel invasion distinguishes the two entities.
Functional changes do not typically occur in follicular thyroid cancer. No laboratory thyroid function test is specific for diagnosis.
Clinically, follicular thyroid carcinoma presents with an asymptomatic thyroid nodule or mass. Pain is not common. More advanced disease can present with vocal cord paralysis, dysphagia, or in 10-15% of patients diffuse metastatic disease.
Imaging for follicular CA includes ultrasound to evaluate the nodule and assess cystic vs. solid features. Ultrasound is also helpful in determining size, invasion of adjacent structures, and directing biopsy. CT scan can be used to evaluate for metastatic disease.
Diagnosis is best made with excisional biopsy and evaluation for pseudocapsule and blood vessel invasion. Cytology is not as helpful in diagnosis of follicular carcinoma due to the similar cell morphology between follicular adenoma and carcinoma cells.
Treatment for follicular thyroid cancer is primarily surgical thyroidectomy with or without neck dissection for lymphadenopathy. Adjuvant therapy for locally or distally invasive disease include radioactive iodine and external beam radiation therapy (EBRT).
Follicular Carcinoma Non Descript Except for Calcifications |
|
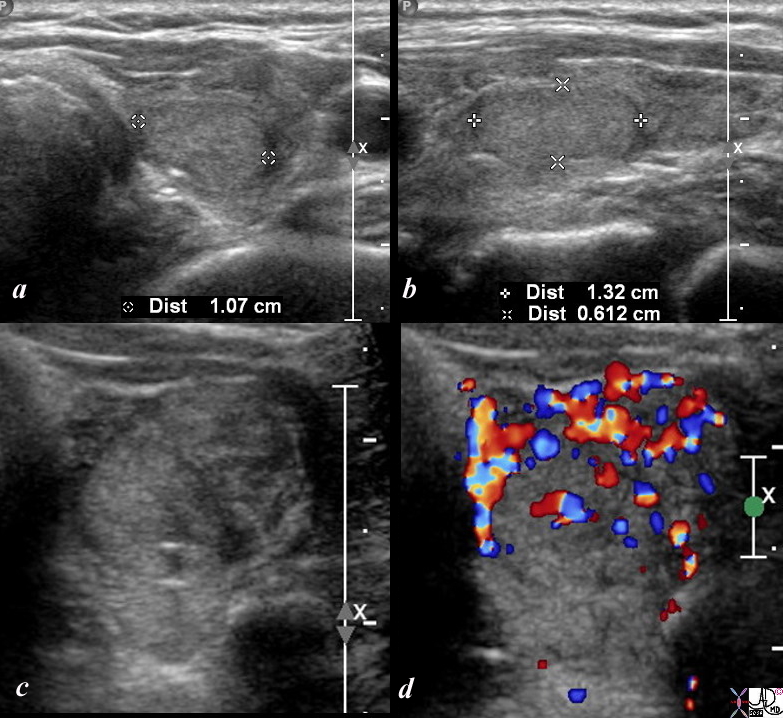
This is a thyroid scan from a 53 year old female with a clinical history of bilateral thyroid nodules. The scan shows a homogeneous nodule in the mid to upper pole of the left lobe that measures 1.1 by 1.3 X .6cms (a,b). On magnification (c) a shadowing calcification is noted associated with mild heterogeneity in the rest of the gland, and demonstrates significant vascularity on Doppler color flow examination. The pathological diagnosis was follicular cell carcinoma. Courtesy Barry Sacks MD Copyright 2010 99390c01.8s |
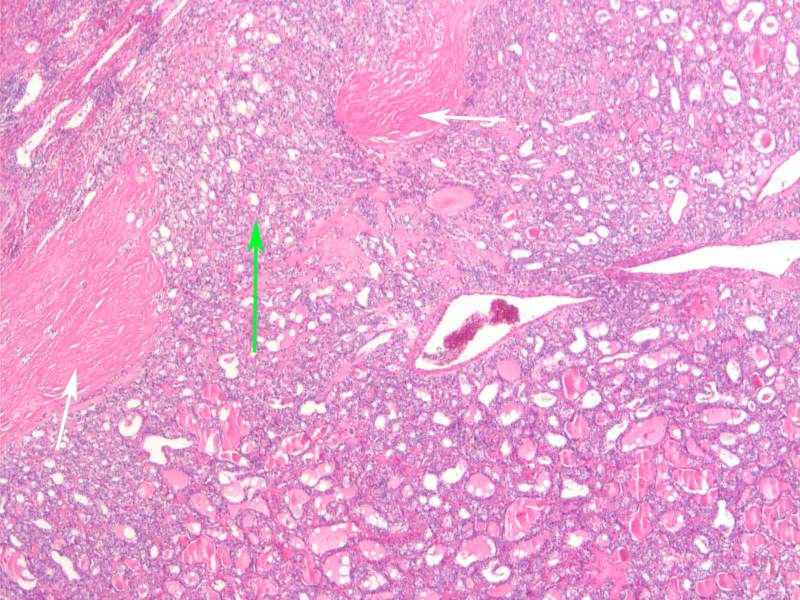
Invasion of the Capsule 4X H&E |
|
The histological section at 4X magnification using H&E stain shows findings consistent with minimally invasive follicular ca with transcapsular invasion carcinoma. The capsule is shown as layers of collagen (white arrows, that has been breached by invading follicular carcinoma (green arrow). Image Courtesy Ashraf Khan MD. Department of Pathology, University of Massachusetts Medical School. 99408.81 |