The Common Vein Copyright 2010
Macrocalcification
Nodular Form
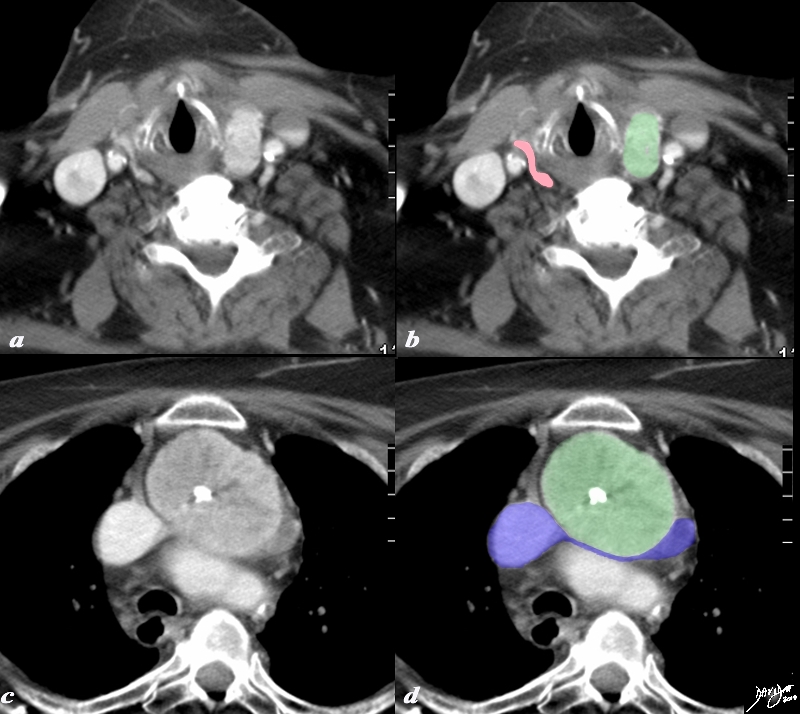
Large Coarse Central Calcification in a retrosternal Goiter |
|
A large retrosternal goiter is seen extending down anterior to the aortic arch and brachiocephalic vein in this 86 year old female patient. In image a and b the atrophied left lobe of the thyroid is overlaid in pink, and the superior aspect of the goiter is overlaid in green. More inferiorly the goiter with central chunky calcification is noted compressing on the brachiocephalic vein (blue) There is mild diffuse almost homogeneous enhancement. The tracheobronchial tree is not affected by this goiter The findings are consistent with a calcified retrosternal thyroid goiter CTscan Courtesy Ashley Davidoff MD Copyright 2010 77978c.8s |
Punctate Form

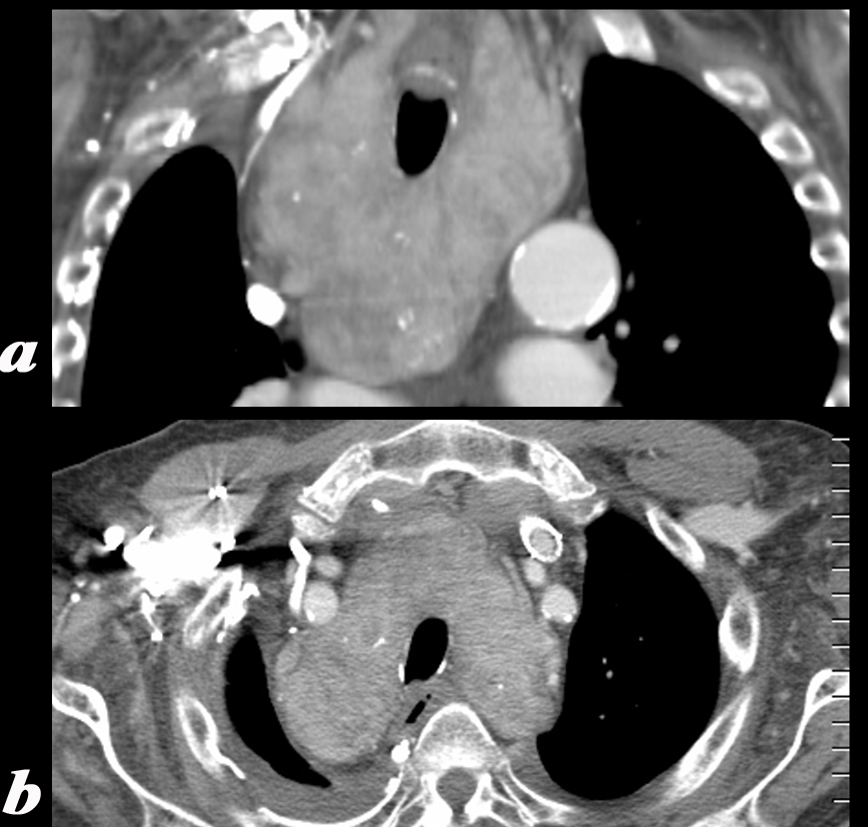
Small Peripheral Coarse Calcification Retrosternal Goiter |
|
The plain film (a), with magnified view (b) shows a large mass shifting and compressing the trachea (teal) to the right. The mass is seen on cross sectional CT as an irregularly enhancing mass connected to the thyroid gland on more cranial views. Its mass effect on the trachea narrowing it in the transverse dimension is well demonstrated. Two small but coarse calcifications are noted in the posterior aspect of the gland as 1mm white concretions. The findings are consistent with a retrosternal thyroid goiter Courtesy Ashley Davidoff MD Copyright 2010 31460c01.81s |
Diffuse Goiter with benign Appearing Calcifications |
|
The CT is from a 75 year old man who has had a goiter for many years. The images reflect diffuse enlargement of the thyroid seen on the coronal view (a) and on an axial scan (b). The gland is enlarged with each lobe measuring about 12 cms in craniocaudad dimension (length) by 6cms in anteroposterior dimension by 12 cms in transverse dimension. The symmetric widening of the mediastinum seen in (a) is unusual for a retrosternal goiter which tends to affect one lobe more than another. Image (a) also shows diffuse enlargement of the gland affecting both sides to almost the same degree, heterogeneously enhancing texture with scattered coarse calcifications, but no obvious discrete nodules except perhaps in the lower lobe on the left. The trachea is narrowed from side to side but is not displaced because of the symmetric involvement which pushes on the trachea from both sides. The enlarged gland maintains its thyroid shape despite the significant changes in size and texture. Image b reveals the same findings in transverse dimension and again shows the symmetric pressure placed on the narrowed trachea A right pleural effusion is noted These findings are consistent with a diffusely involved goiter. Courtesy Ashley Davidoff MD Copyright 2010 94714c02 |
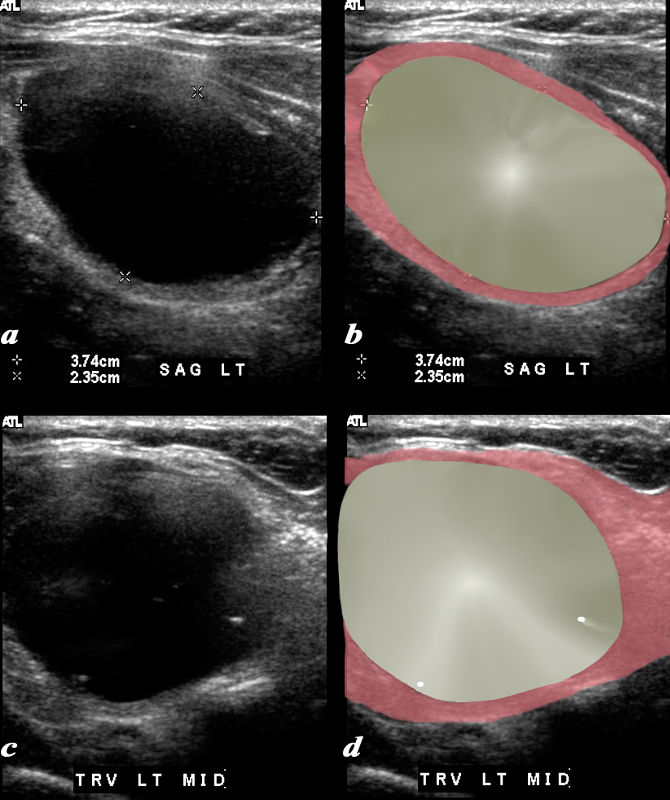
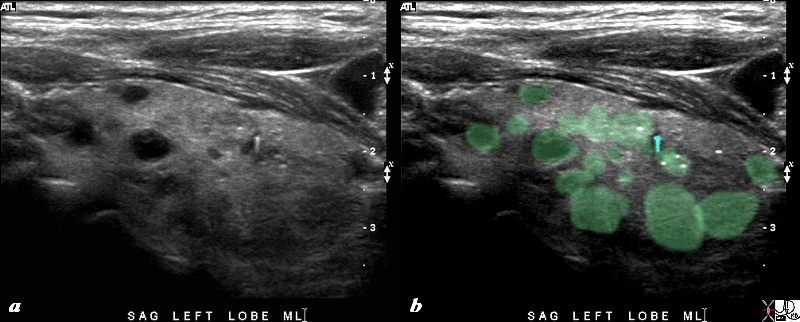
Small Calcifications in a Large Cyst |
|
A large cyst occupies almost the entire left lobe of the thyroid gland is seen by ultrasound which in sagittal (a,b) measures 3.7cms and in A-P dimension measures 2,4cms(c,d). The cyst is characterised by anechogenicty, through transmission but no definite back wall enhancement. Two small calcifications are seen as white specks in the transverse view. The gland is compressed (salmon pink). These findings are characteristic of a large simple cyst of the gland. Courtesy Barry Sacks MD Copyright 2010 97018c01.8 |
Curvilinear Macrocalcification
|
Curvilinear and Coarse Calcerification – Retrosternal Gioter |
|
A large retrosternal goiter is seen extending down behind the aortic arch. The calcifications within suggest an outline of a large nodule with both curvilinear fine calcification as well as chunky calcification. Its mass effect on the trachea is noted. The trachea is pushed toward the right and is minimally compressed. The findings are consistent with a calcified retrosternal thyroid goiter Courtesy Ashley Davidoff MD Copyright 2010 31504.8 |

|
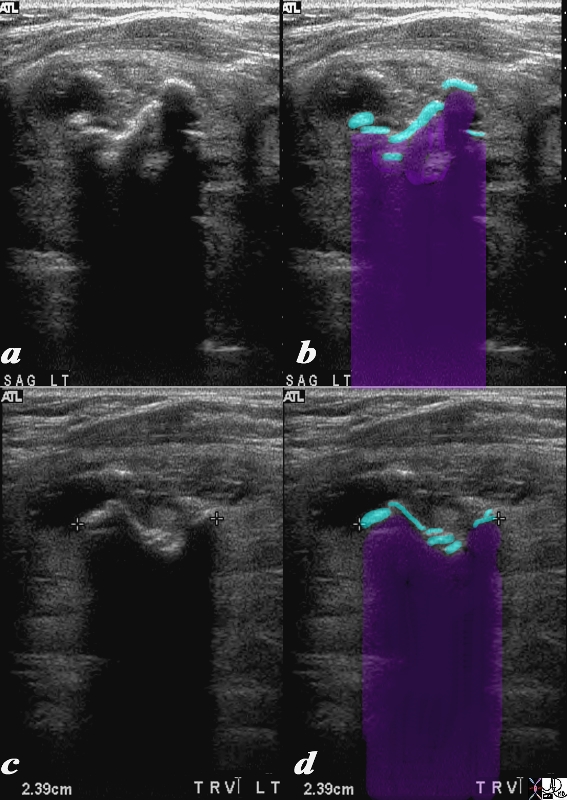
Curvilinear Shadowing Macrocalcification |
|
This 74year old female presents with a multinodular goiter. Images are taken in sagittal (a,b) and transverse (c,d). Multiple macrocalcifications (teal blue in b and d) preclude visualization of the gland because of extensive calcifications resulting in shadowing (black in a and c – purple in b and d) of the remaining thyroid parenchyma. These findings are consistent with a benign non toxic multinodular thyroid gland. The macrocalcifications are characteristic of benign disease. Courtesy Ashley Davidoff MD Copyright 2010 95706c.8s |
Microcalcification
Microcalcification with Ring Down or Comet TAil – Considered a Benign Feature |
|
The 80 year old male presents with an asymptomatic multinodular goiter, consisting many nodules of varying size and echogenicity, as seen by sagittal A microcalcification with ring down artifact is seen overlaid in teal blue. Other microcalcifications are probably present (overlaid in white). The multiple nodules that are not border forming are within the confines of the parenchyma and do not alter the shape of the gland. The right lobe of the thyroid measures about 4.5 cms in sagittal 1.5cms.in A-P dimension, and 1.5cms in the transverse plane. The gland is therefore not enlarged These findings are consistent with a non toxic multinodular thyroid gland, and not truly a goiter since the gland is not enlarged. The ringdown or comet tail artifact characteristic of small calcifications is exemplified in this image and is usually a sign of benign calcification. On the other hand the fine echogenicities without ring down artifact are more concerning. Courtesy Ashley Davidoff MD Copyright 2010 94780c06L.8s |
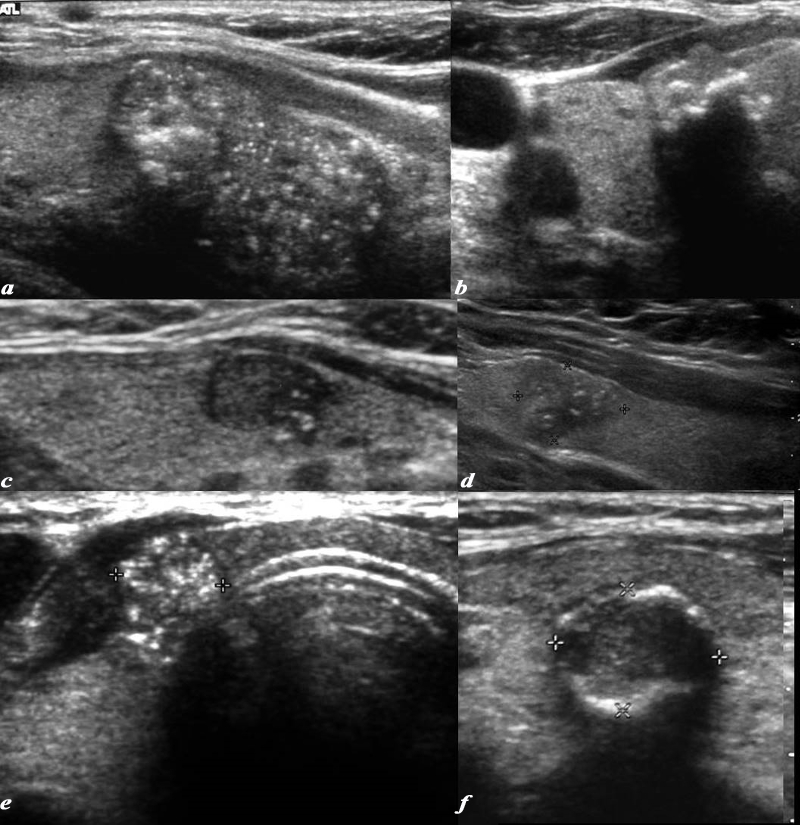
Range of Microcalcifications in Papillary Carcinoma |
|
This series of ultrasounds reveal patients with papillary carcinoma showing the range of calcifications. They include the non shadowing, non comet tail, echogenic foci seen in images a,c,d,e, and macrocalcifications of shadowing calcifications (images b and f) code thyroid character nodule fx nodules calcification microcalcification non shadowing dx non functioning non functional diagnosis papillary carcinoma USscan ultrasound Courtesy Barry Sacks MD Copyright 2010 97203ec03.8L |
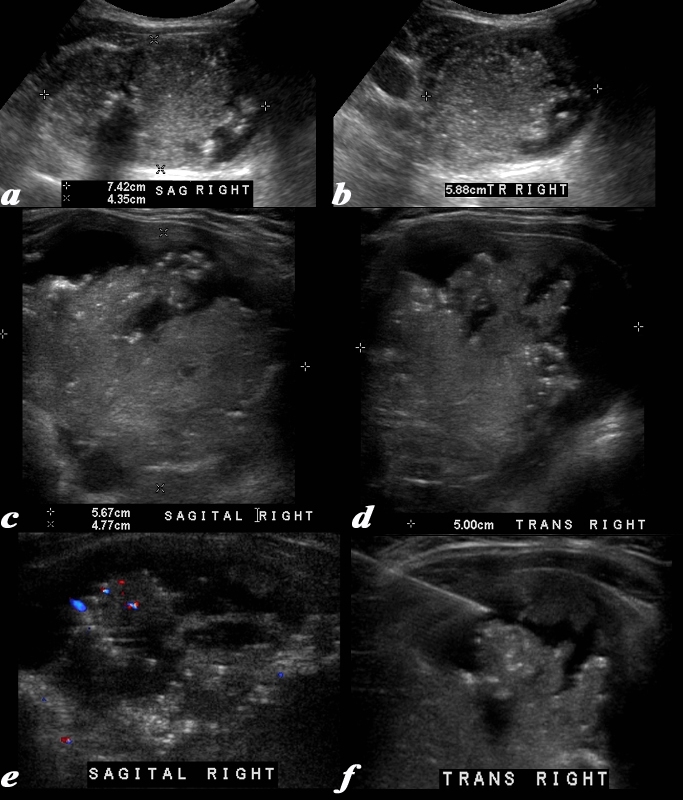
Microcalcifications – Papillary Carcinoma |
|
This 63 year old male presents with an enlarged thyroid Ultrasound shows a mass in the right lobe of the thyroid. The right lobe measures 7.4cms in sagittal (a), 4.4 cms in A-P dimension (a) and 5.9cms in transverse view A complex mass is noted in the right lobe. with innumerable small echogenic foci consistent with non shadowing microcalcifications. High resolution imaging of the mass using a linear transducer shows the mass to consist of fronds of tissueand the microcalcifications nare better visualized. The mass measures 5.7cms in sagittal (c) and 5 cms in transverse view (d). Doppler study shows hypovascularity (e) and image f shows a biopsy needle in close proximity to the microcalcifications. A diagnosis of papillary carcinoma was made based on the biopsy Courtesy Ashley Davidoff MD Copyright 2010 96145c.8L |
Psammomatous Calcifications in Papillary Carcinoma |
|
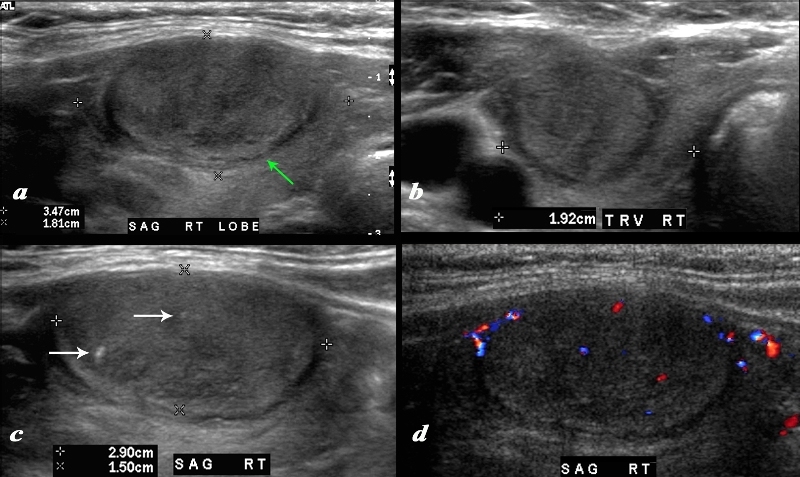
A large nodule in the thyroid occupies almost the entire right lobe (a). The nodule measures 2.9cms by 1.5cms. The gland is not enlarged and measures 3.5cms (craniocaudad), by 1.8cms (A-P) by 2.4cms (transverse). The nodule is almost isoechoic with normal thyroid but shows internal irregular areas of hypoechogenicity, regions of isoechogenicity, as well as microcalcifications (white arrows (c). There is irregularity of the border at the posterior aspect of the nodule green arrow a). The halo shows irregular borders in this region as well. Internal vascularity is minimal (d). The irregular surface is concerning for a malignant processes. The diagnosis in this patient was papillary carcinoma Courtesy Ashley Davidoff MD Copyright 2010 74909c02L.8 |
Medullary Carcinoma Microcalcifications |
|
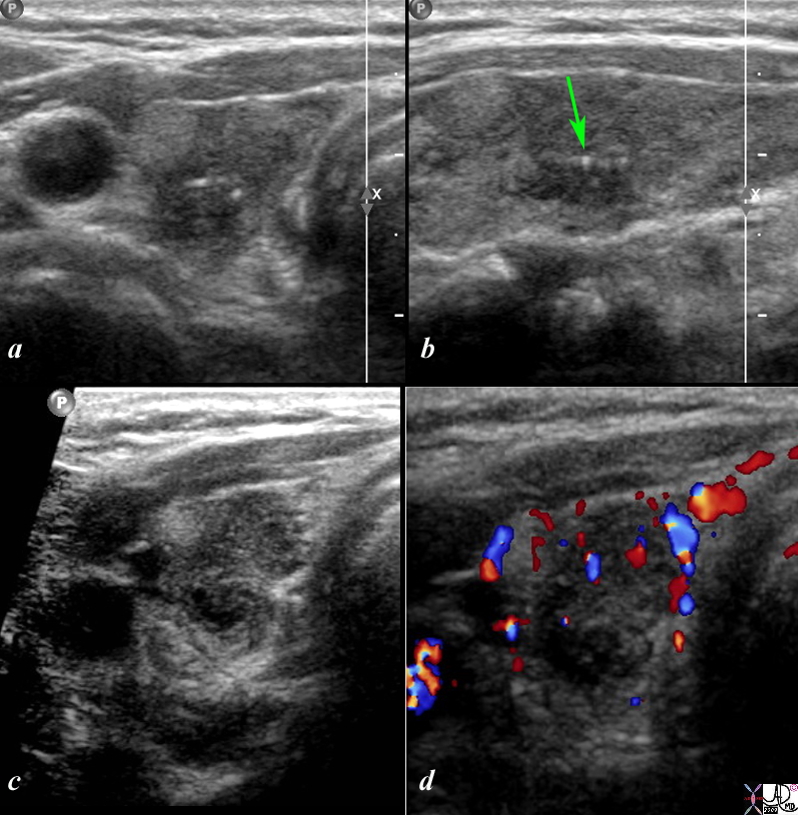
This is a thyroid scan from a 53 year old female with a clinical history of bilateral thyroid nodules. The scan shows a heterogeneous nodule in the mid to upper pole of the right lobe that is ill defined both on the transverse view (a) as well as the sagittal view (b). An echogenic nodule is part of the complex lesion. In addition non-shadowing microcalcifications with ring down (green arrow) are seen in both the transverse view (a) and sagittal view (b). On magnification and more contrasted settings the heterogeneity of the lesion is further demonstrated and low vascularity is shown on the Doppler interrogation (d). The pathological diagnosis was medullary cell carcinoma. Courtesy Barry Sacks MD Copyright 2010 99389cL.8s |
Calcification in Cervical Lymph Nodes Metastattic Papillary Carcinoma |
|
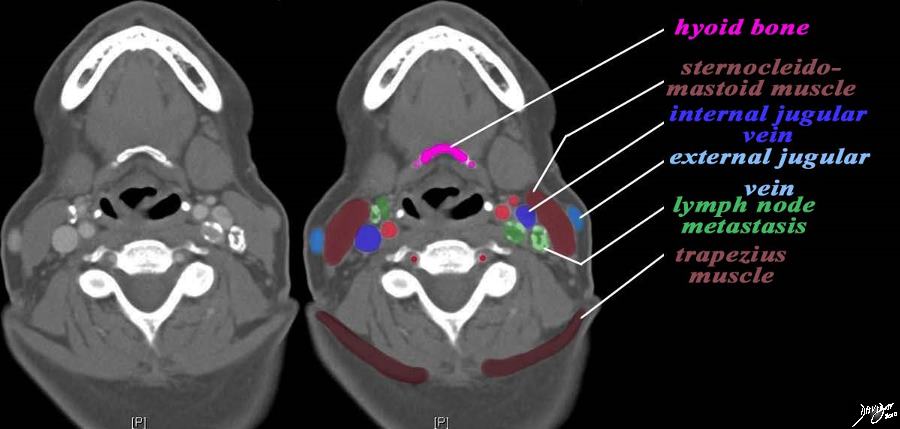
The CT scan is from a middle aged female patient with metastatic papillary carcinoma of the thyroid. her nodes contain calcification and hence are easily seen. The case exemplifies the metastatic lymph node pattern of thyroid carcinoma. The most superior cut is at the level of the hyoid bone (pink). At this level the nodes associated with the internal jugular vein (royal blue) are the upper cervical nodes. These are posterior to the internal vein on the left and anterior on the left (dark green) There are no nodes associated with the external jugular vein nor in the posterior triangle which lies between the sternocleidomastoid muscle anteriorly and the trapezius posteriorly (maroon). Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 93812c14.9s |