The Common Vein Copyright 2010
Introduction
The the most important dimension when considering enlargement of the gland is the A-P diameter which should not be >2cms. The length is considered large when in the 4-6cms range and trannsverse should not be larger than 2.8cms.
The small gland is measures lesss than 4 cms inlength, less than 2cms wide, and less than 1cms thick.
Non Toxic vs Toxic
A clinically approach to the large thyroid is to divide the entity based on whether there is evidence of hyperfunction normal or hypofunction.
Non Toxic Goiter

Single Nodule Causing Enlarged Gland |
|
The diagram illustrates a single non toxic nodule that causes the gland to become enlarged by virtue of its individual size. This nodule could be benign or malignant. Courtesy Ashley Davidoff MD Copyright 2010 93852e07h03.8s |
Large Retrosternal Goiter Left Lobe Enlrgement Normal Right Lobe |
|
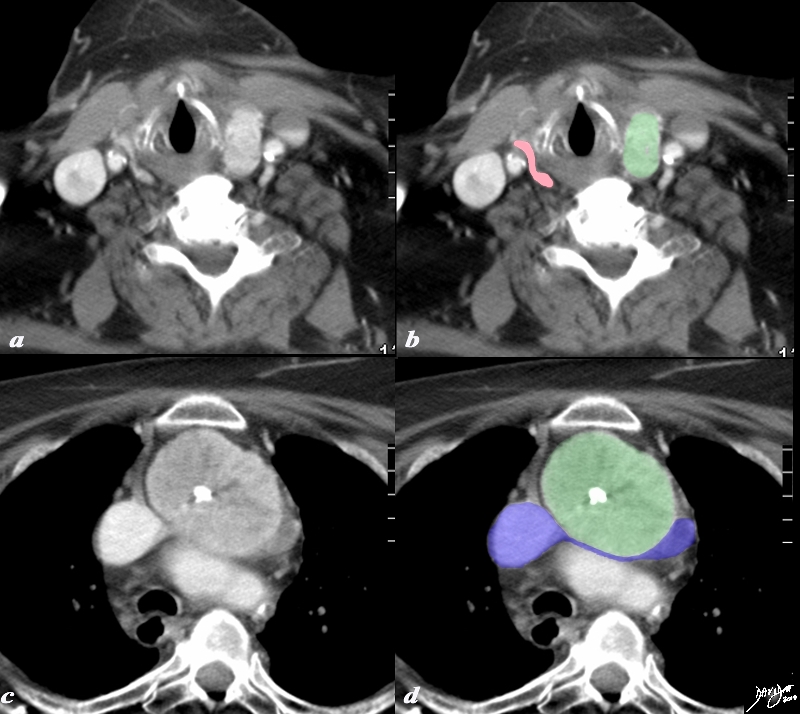
A large retrosternal goiter caused by an abnormal left lobe is seen extending down anteriorly to the top aortic arch is noted in this 74 year old female patient. The normal right lobe is seen overlaid in pink (d) lateral to the trachea (teal). In image a and b the visualized portion of the goiter measures 8.8cms, has a central avascular component and an enhancing rind. The goiter is overlaid in green and seen displacing the trachea (teal blue) to the right. On the axial cuts the goiter with central avascularity is again noted compressing on the trachea and pushing it to the right (teal blue) the esophagus is also pushed rightward. The brachiocephalic vein (blue) is compressed and there are venous varicosities both on the left and posteriorly on the right of the goiter. Anterior chest veins are also prominent. The findings are consistent with a retrosternal thyroid goiter caused by an enlarged left lobe. Courtesy Ashley Davidoff MD Copyright 2010 94516c.8s |
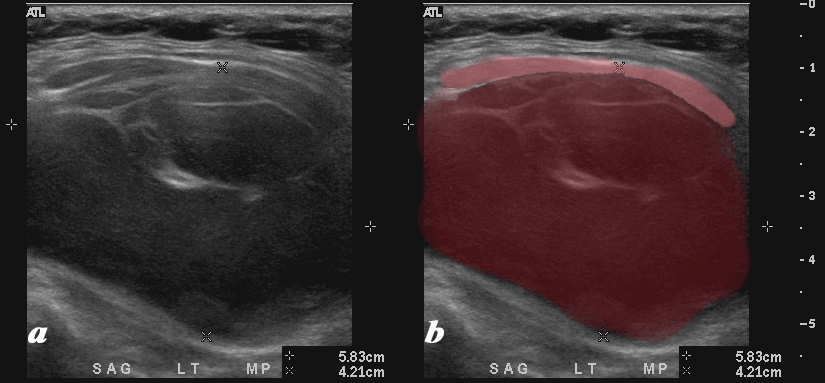
Hemorrhagic Cyst Causing Enlargement of the Whole Gland |
|
A large mostly hypoechoic mass expands the left lobe of the thyroid on the ultrasound of this 54 year female who presents with an enlarged thyroid gland. The left lobe is filled with low level echoes and contains multiple thin septal echogenic walls (maroon). The mass appears to displace and compress normal soft tissues of the neck (pink) anteriorly. Doppler showed no flow. The mass occupies the entire left lobe and measures 5.8cms in craniocaudad span and by 4.2 cms transversely The diagnosis in this patient is a hemorrhagic cyst causing a goiter. Courtesy Ashley Davidoff MD Copyright 2010 94656c01L |
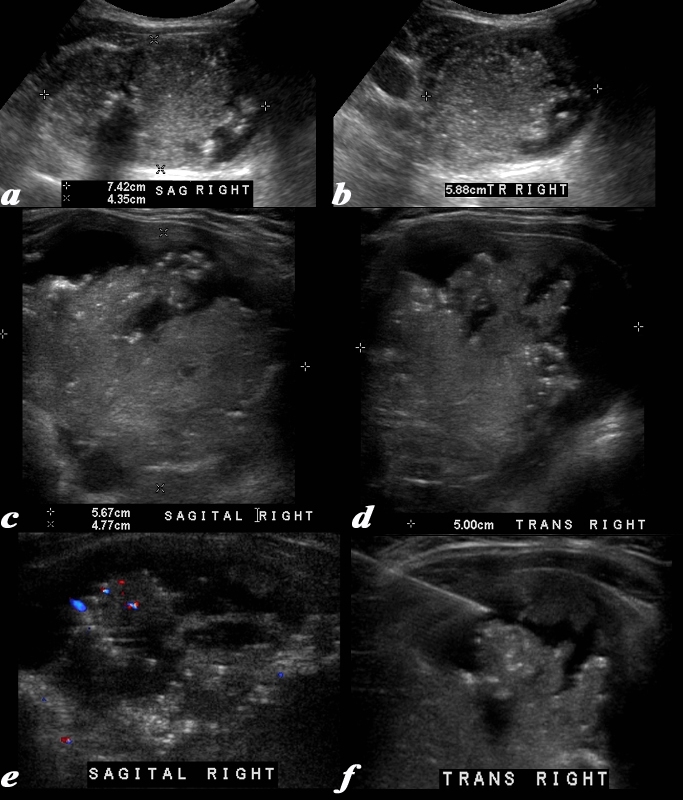
Malignant Goiter – Papillary Carcinoma |
|
This 63 year old male presents with an enlarged thyroid Ultrasound shows a mass in the right lobe of the thyroid. The right lobe measures 7.4cms in sagittal (a), 4.4 cms in A-P dimension (a) and 5.9cms in transverse view A complex mass is noted in the right lobe. with innumerable small echogenic foci consistent with non shadowing microcalcifications. High resolution imaging of the mass using a linear transducer shows the mass to consist of fronds of tissueand the microcalcifications nare better visualized. The mass measures 5.7cms in sagittal (c) and 5 cms in transverse view (d). Doppler study shows hypovascularity (e) and image f shows a biopsy needle in close proximity to the microcalcifications. A diagnosis of papillary carcinoma was made based on the biopsy Courtesy Ashley Davidoff MD Copyright 2010 96145c.8L |
Enlargement Due to Multinodular Goiter – A Knobbly Gland
Non Toxic Multinodular Goiter |
|
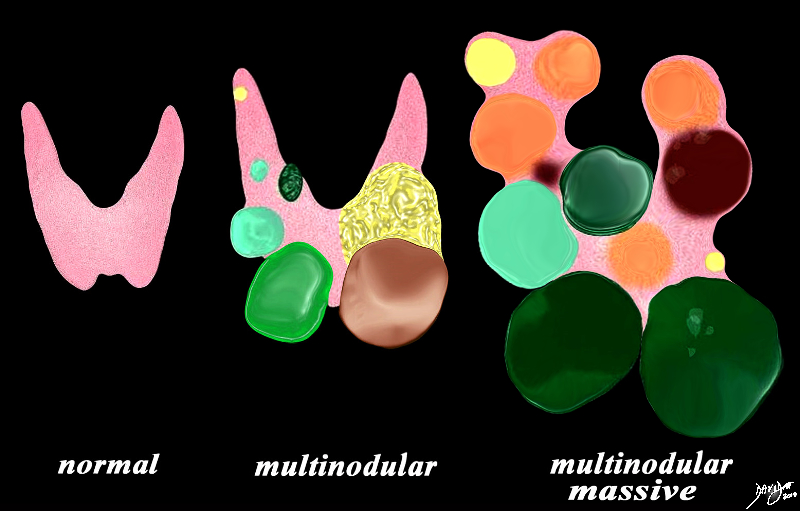
The diagram illustrates non toxic multinodular goiter together with a normal thyroid gland on the left. A moderately enlarged gland (middle) containing multiple variably sized non toxic nodules with different characteristics is shown together with a massively enlarged non toxic gland (right) When the gland becomes massively enlarged it may extend into the chest, compress the airway and neck veins as well as displace other structures such as the esophagus. Courtesy Ashley Davidoff MD Copyright 2010 93852e07h01a03.8s |

The Retrosternal Goiter |
|
The plain film (a), with magnified view (b) shows a large mass shifting and compressing the trachea (teal) to the right. The mass is seen on cross sectional CT as an irregularly enhancing mass connected to the thyroid gland on more cranial views. Its mass effect on the trachea narrowing it in the transverse dimension is well demonstrated. The findings are consistent with a retrosternal thyroid goiter CTscan Courtesy Ashley Davidoff MD Copyright 2010 31460c01.8s |

Heterogeneity of Multinodular Goiter |
|
The multinodular goiter in this diagram is a combination of simple cysts (yellow), complex cysts (light green) and solid nodules (dark green). Characterisation of complex and solid lesions is best first evaluated by ultrasound but will usually require fine needle aspiration and microscopic evaluation when suspicious lesions are identified. Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 93852.d13.8s |
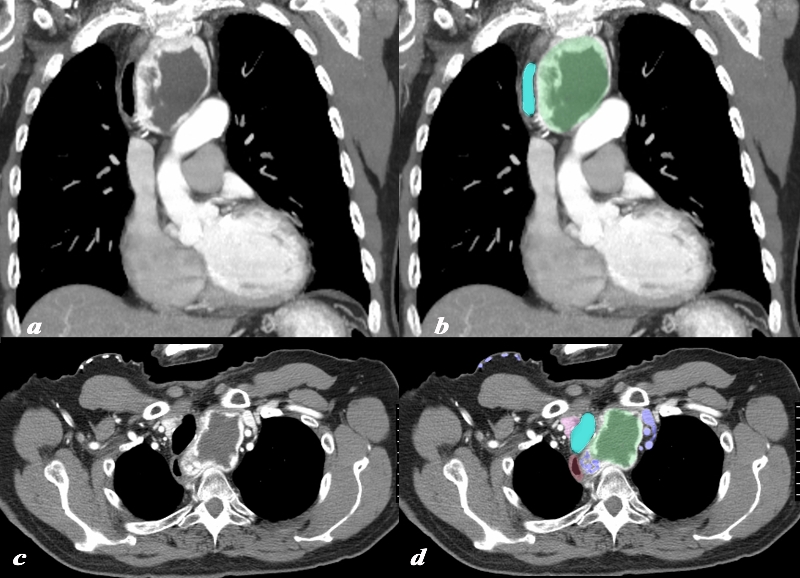
Retrosternal Goiter Compressing the Brachiocephalic Vein |
|
A large retrosternal goiter is seen extending down anterior to the aortic arch and brachiocephalic vein in this 86 year old female patient. In image a and b the atrophied left lobe of the thyroid is overlaid in pink, and the superior aspect of the goiter is overlaid in green. More inferiorly the goiter with central chunky calcification is noted compressing on the brachiocephalic vein (blue) There is mild diffuse almost homogeneous enhancement. The tracheobronchial tree is not affected by this goiter The findings are consistent with a calcified retrosternal thyroid goiter Courtesy Ashley Davidoff MD Copyright 2010 77978c.8s |
|
Retrosternal Goiter with Central Avascularity and Compressing the Brachiocephalic Vein |
|
A large retrosternal goiter is seen extending down anterior to the top aortic arch is noted in this 74 year old female patient. In image a and b the visualized portion of the goiter measures 8.8cms, has a central avascular component and an enhancing rind. The goiter is overlaid in green and seen displacing the trachea (teal blue) to the right. On the axial cuts the goiter with central avascularity is again noted compressing on the trachea and pushing it to the right (teal blue) the esophagus is also pushed rightward. The brachiocephalic vein (blue) is compressed and there are venous varicosities both on the left and posteriorly on the right of the goiter. Anterior chest veins are also prominent. The findings are consistent with a retrosternal thyroid goiter Courtesy Ashley Davidoff MD Copyright 2010 94516c.8s |
Diffuse Enlargement
Diffuse Enlargement – Subacute Thyroiditis |
|
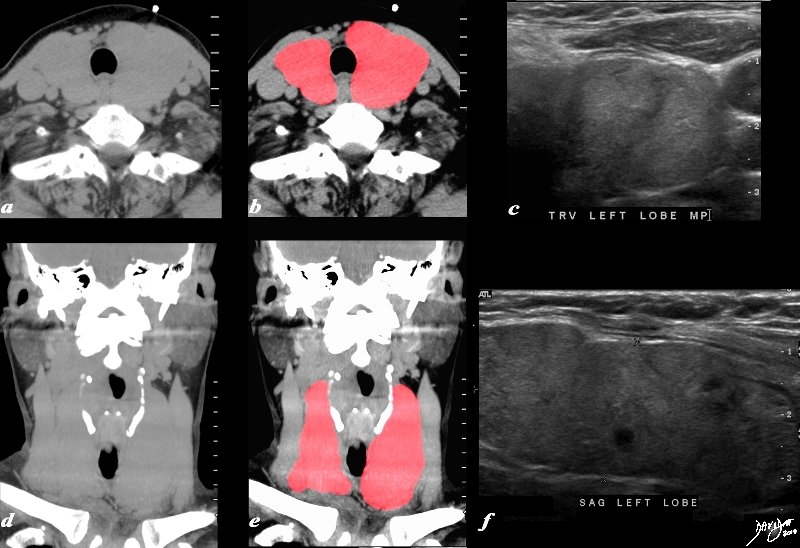
A diffusely enlarged almost homogeneous thyroid gland is seen in the non contrast CTscan of this 78 year old female patient. (a,b,d,e) The thyroid gland measures 8.5cms (craniocaudad), by 3.9cms (A-P) by 4.8cms (transverse). Clinical findings were consistent with subacute thyroiditis, with biochemical findings suggesting hypothyroidism. The ultrasound (c,e) shows an enlarged gland as well with similar dimensions, appearing almost round on the transverse view (c). This rounded shape in the transverse dimension is a clue to the presence of a large and abnormal gland, even before the measurements are evaluated. The gland is mildly heterogeneous particularly well seen on the sagittal view (e). The findings are consistent with a thyroiditis. Courtesy Ashley Davidoff MD Copyright 2010 94549c04L.8s |

Diffuse Enlargement |
|
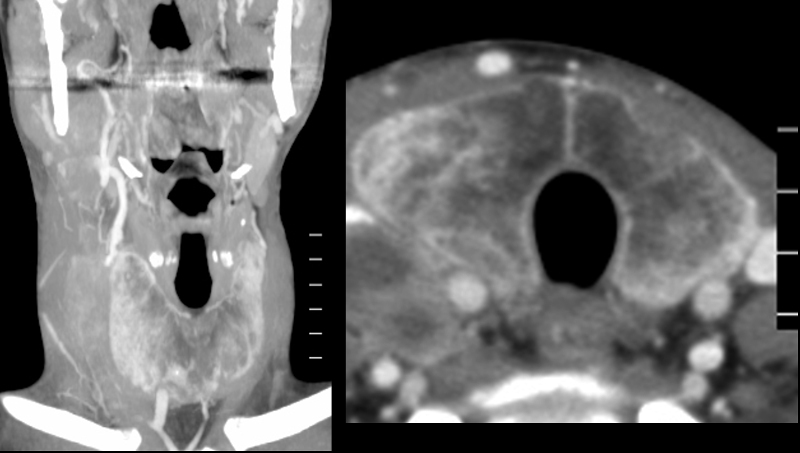
The CT is from a 75 year old man who has had a goiter for many years. The images reflect diffuse enlargement of the thyroid seen on the scout CXR prior to a CT scan, on the coronal view (b,c) and on an axial scan. The gland is enlarged with each lobe measuring about 12 cms in craniocaudad dimension (length) by 6cms in anteroposterior dimension by 12 cms in transverse dimension. The symmetric widening of the mediastinum seen in (a) is unusual for a retrosternal goiter which tends to affect one lobe more than another. Image (b) shows diffuse enlargement of the gland affecting both sides to almost the same degree, heterogeneous in texture with scattered coarse calcifications, but no obvious discrete nodules. The trachea is narrowed from side to side but is not displaced because of the symmetric involvement which pushes on the trachea from both sides. Image c shows the enlarged gland which maintains its thyroid shape, and again shows heterogeneous enhancing texture with scattered coarse calcifications. Image d reveals the same findings in transverse dimension and again shows the symmetric pressure placed on the narrowed trachea These findings are consistent with a diffusely involved goiter. Courtesy Ashley Davidoff MD Copyright 2010 94714c01.8 |
Amyloidosis of the Thyroid |
|
The CT is from a 35 year old man with a complex history including long standing history of Crohn’s disease and a recent history of lymphoma. He has had a goiter for many years and biopsy showed amyloidosis of the thyroid. The image on left is a coronal view of the neck and the b is a transverse view of the thyroid. The gland is enlarged measuring 6.2cms in Craniocaudal dimension (length) by 3cms in anteroposterior dimension by 3cms in transverse dimension. On the transverse view it is not quite round but the gland is full bodied reminiscent of its large size. The density appearance is puzzling. Since no non contrast CT was performed the peripheral increase in density may be due to enhancement or more likely due to iodine or calcification. The soft densities to the right of the right lobe are related to the patients newly diagnosed lymphoma. Courtesy Ashley Davidoff MD Copyright 2010 94553c.8 |
Goiter with Hyperthyroidism

Hyperthyroidism (right) and Normal (left) |
|
Patients with hyperthyroidism may have diffuse enlargement of a hyperfunctioning gland as seen in the right image (red). The left image (pink) is a normal gland. The enlargement may be due to Graves disease or thyroiditis. Courtesy Ashley DAvidoff MD copyright 2010 all rights reserved 93852.d03c.8s |
Cause of Toxic Goiter |
|
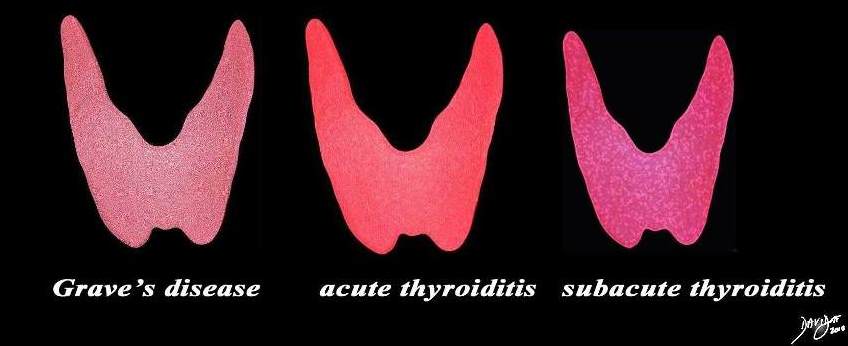
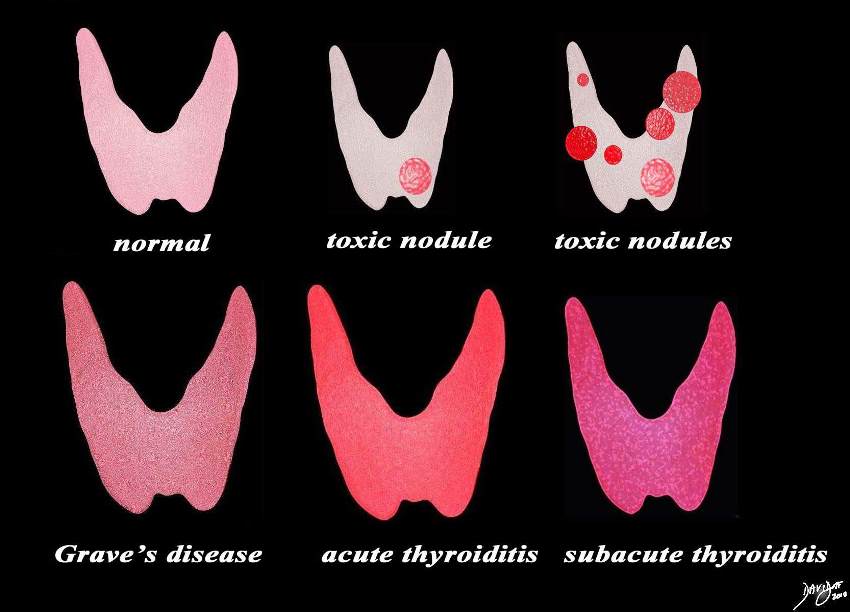
The enlarged smooth gland The enlarged smooth gland is usually seen in patients with thyroxicosis and includes Grave’s disease, acute thyroiditis and subacute thyroiditis This diagram shows the structural possibilities in a patient who presents with thyrotoxicosis Reading from upper left the normal thyroid is shown for reference of size and normal activity (pink) Next is the single toxic nodulke that suppresses the function of the gland and the also causes the gland to shrink. This is followed by a diagram of multiple toxic nodules and the gland in this case may also be smaller or larger than normal depending on the size of the nodules. The lower series of images include Grave’s disease which is the most common cause of thyrotoxicosis, followed by acute thyroiditis and then subacute thyroiditis. Image Ashley DAvidoff MD copyright 2010 all rights reserved 93852.d03cdc06.8s |

|

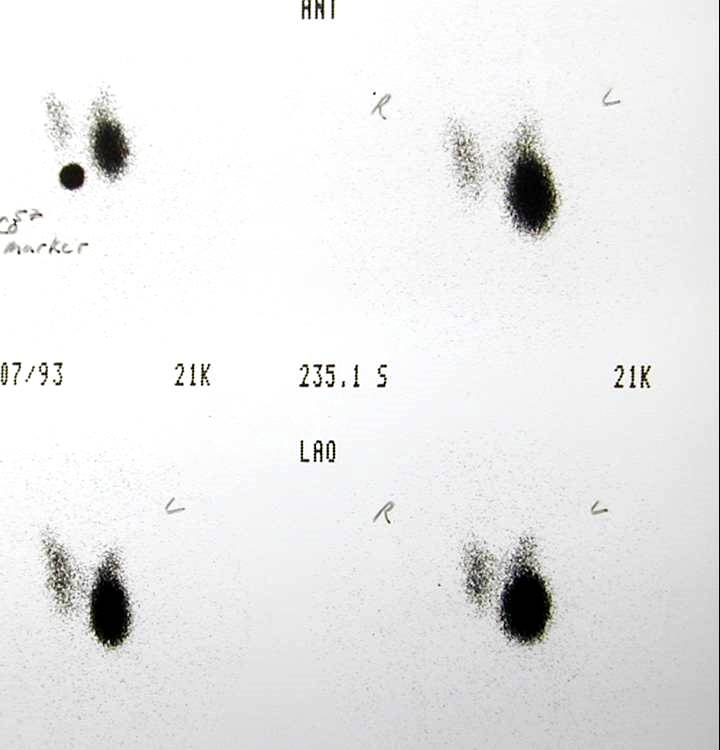
Goiter with Single Hot Nodule |
|
The patient presents with hyperthyroidism and a thyroid scan shows a hot nodule in the lower pole of the left lobe. This finding is consistent with a toxic nodule with suppression of th remaining gland Image Courtesy Barry Sacks MD 99422 |